Research Article
Endogenus toxicology: Modern physio-pathological aspects and relationship with new therapeutic strategies. An integrative discipline incorporating concepts from different research discipline like Biochemistry, Pharmacology and Toxicology

Luisetto M1*, Naseer Almukhtar2, Behzad Nili Ahmadabadi3, Gamal Abdul Hamid4, Ghulam Rasool Mashori5, Kausar Rehman Khan6, Farhan Ahmad Khan7 and Luca Cabianca8
1Applied Pharmacologist, Independent Researcher, Italy2College of Medicine, University of Babylon, Hilla, Iraq
3Innovative Pharmaceutical Product Development Specialist, USA
4Hematology Oncology, University of Aden, Aden, Yemen
5People University of Medical & Health Sciences for Women, Nawabshah, Pakistan
6Preston University Karachi, Pakistan
7Department of Pharmacology Government Medical College, Shahdol, M.P, India
8Biomedical Labo, HYPERLINK, Italy
*Address for Correspondence: Luisetto M, Applied Pharmacologist, Independent Researcher, Italy, 29121 Email: [email protected]
Dates: Submitted: 29 December 2018; Approved: 11 January 2019; Published: 14 January 2019
How to cite this article: Luisetto M, Almukhtar N, Ahmadabadi BN, Hamid GA, Mashori GR, et al. Endogenus toxicology: Modern physio-pathological aspects and relationship with new therapeutic strategies. An integrative discipline incorporating concepts from different research discipline like Biochemistry, Pharmacology and Toxicology. Arch Cancer Sci Ther. 2019; 3: 001-024. DOI: 10.29328/journal.acst.1001004
Copyright License: © 2019 Luisetto M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Endogenous toxicology; Physiology; Pharmacological strategies; New pathogenetic theories; Cancer; Metastasys

Abstract
Many pathologic disease can be considered as related to an Endogenous toxicological moves and in time dependent way (kinetics and dynamic of the process). In this work starting from the analysis of relevant literature involved with different disease and related to the endogenous local micro- environment some global conclusion useful as new tools for innovative pharmacological strategies will be submitted to the researcher. Physiology, pathology concept linked to the endogenous toxicological local micro-environment status as new research instruments. The same carcinogenesis process can be related also to endogenous agents that may have a major contribution in spontaneously process. (Reactive oxygen species (ROS), which are involved in multiple cellular processes by physiologically transporting signal as a second messenger or pathologically oxidizing DNA, lipids, and proteins).
Introduction
Human poisons substantives are universally classified from exogenous origin as from mineral world or from plants or from animal origin. But In the poison of animal origin we can include also some endogenous substantia as methabolic–catabolic molecule or other Situation that can produce a toxicant effect. According IUPAC Glossary of Terms Used in Toxicology, 2nd Edition IUPAC Recommendations, 2007 Endogenous term (antonym of exogenous) mean produced within or caused by factors within an organism. So, is possible to observe under and endogenous point of view some pathological phenomena under a specific endogenous toxicological approach in order to verify if possible new therapeutic option.
Some specific condition can help in right understanding of this new kind of concept: First of all why in human brain are present lots of receptor for some plants drugs? Can we think to an interaction between environment and human phisio- anatomic development and evolution? Why some receptor are strictly related whit agonist – antagonist in example in a SAR structure-activity relationship? Is a real peculiarity (Figure 1). If we observe with a medicinal chemistry approach for example morfin drugs we can easily see a definite receptor with various chemical groups that link exactly with the morfin drugs (form plant world). Is possible to think that some toxic environmental external substances have influenced the human evolutions?
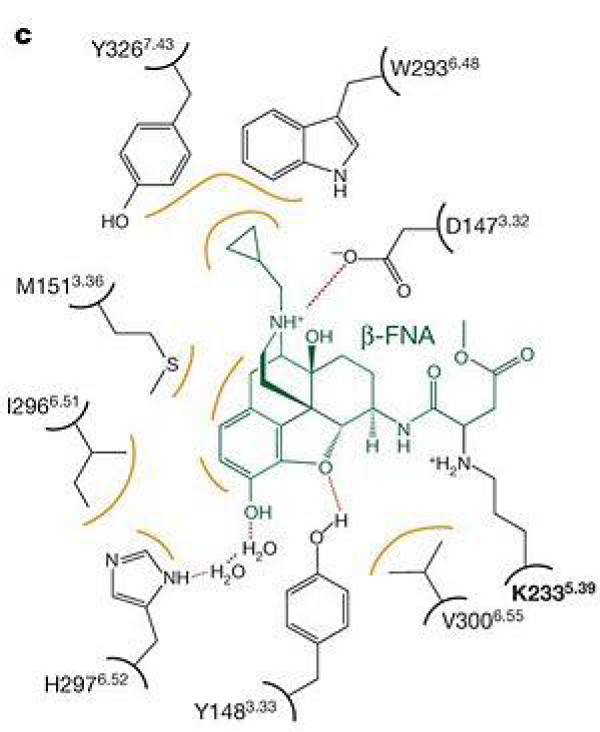
Figure 1: Consistency of rank-ordering between the IN and OUT positions for assessing %BF using hand-held BIA.
Other interesting example can be the endocannabinoid ANANDAMIDE and the cannabinoids receptor related to THC involve in process like Analgesia, antiinflammatory, immune modulators (Figures 2,3).
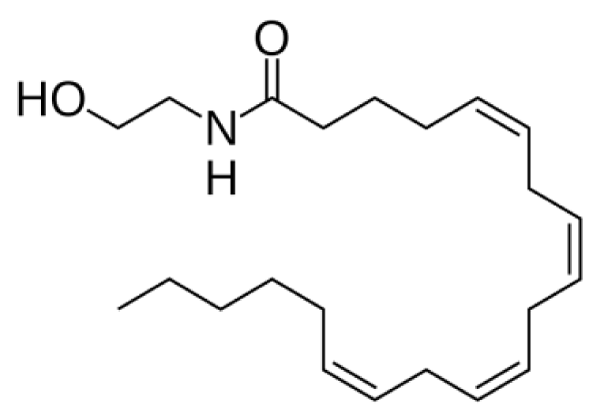
Figure 2: Anandamide Endocannabinoids.
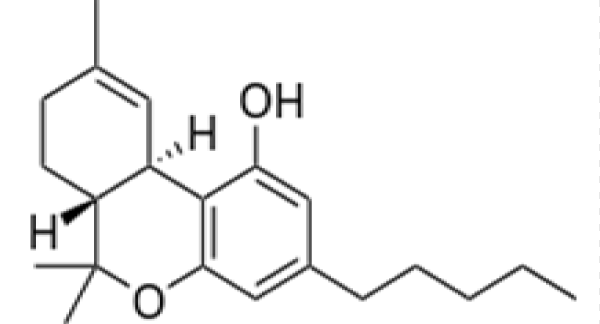
Figure 3: THC Tetrahydrocannabinol.
Interesting examples involved in esogenous or endogenous toxic moves can be some pathologies like:
Taupaty ,Dementia, beta amiloidosis, alzheimer , substantia nigra pathology in some kind Parkinson disease ,that can be observed under an exogenous- endogenous toxicological aspect. (In example see West pacific foci of ASL/PD). The Relationship between West pacific foci of ASL/PD and the annonacea toxins from Annona muricata L. seems involved with results of production of neuronal inclusion (Figure 4), (Is possible to observe a strictly relationship between some plant origin catabolic molecules and nervous system receptor and neurons in a sort of endogenous poisoning caused by metabolic products of this natural toxins, esogenous toxins but also by related catabolic products).
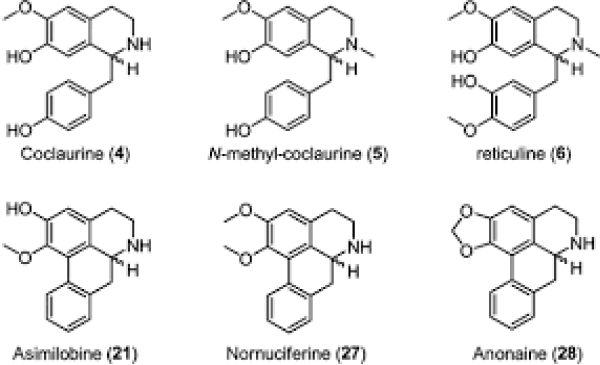
Figure 4: Annonaine Structure.
Some kind of CHF, Diabetes type II (Figure 5) and Iperlipemia, Atherosclerosis (Figure 6) and cardiovascular pathology and other related to methabolic disease with gather of different molecules like glucosilated products, lipids, peroxidated substrated and other. (In all this cases the toxicological moves comes not only from outside but also by an inside methabolism like peroxidate lipids). Also some Immuno -disease and the autoimmunity phenomena can be interesting models to be analized. An immune response versus some endogenous structures even also started by external stimulus (like viruses, bacteria and other). Other interesting pathology for this research to be observed can be heart attack and stroke secondary by acute vessel inflammation and atherogenic process. (Macrophages, lipoproteins, smooth cells, collagens, foam cells, calcium salts, platelet role and other) (Figure 5). Since from the characteristic pattern of some hair loss due to hair follicle death, to some migraine presentation, Alzheimer disease (Figure 7), Parkinson PD, cerebral ictus or to the nerve death in diseases like SMA spinal muscular atrophy, death of retina in opthalmological diseases to blindness a topographic relationship can be observed (inside all the tissue involved). Amyloidosis (Figure 8) and Iperkaliemia (Figure 9). Rheumatic cardiopathy (immunomediated) (Figure 10), Thromboembolic disease, Septic shock, Epilepsy, Cathecolamine iperproduction, Peptic ulcera retaled to high stressing condition, chronic disease and many other conditions can be interesting to be observed under a local micro-environmental process.
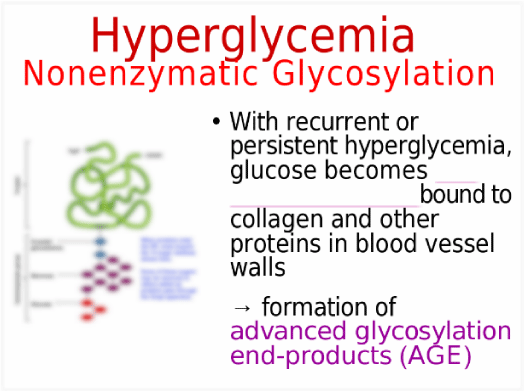
Figure 5:
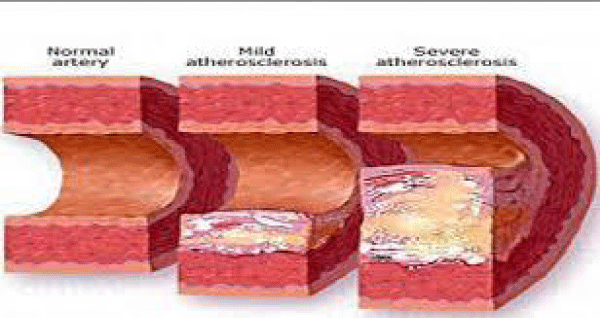
Figure 6: Vessel Atherosclerosis.
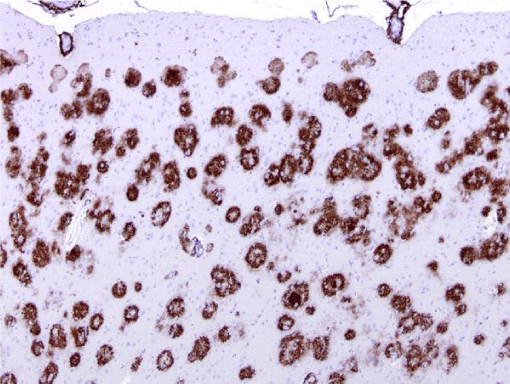
Figure 7: Alzheimer disease brain istology.
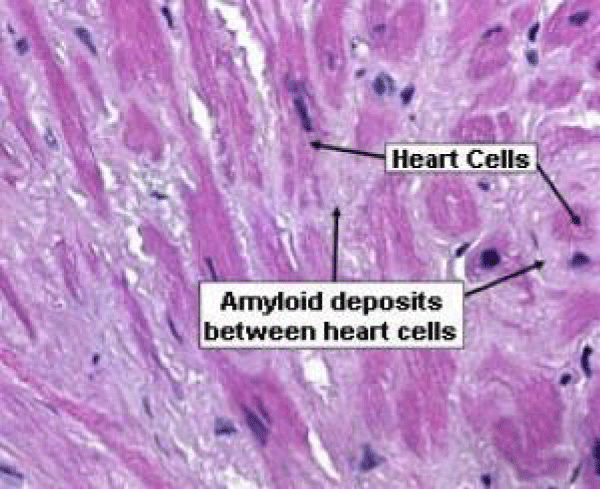
Figure 8: Cardiac amiloidosys.
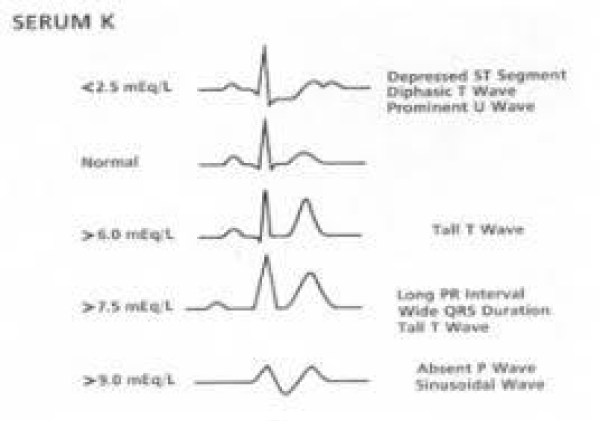
Figure 9: Cardiac amiloidosys.
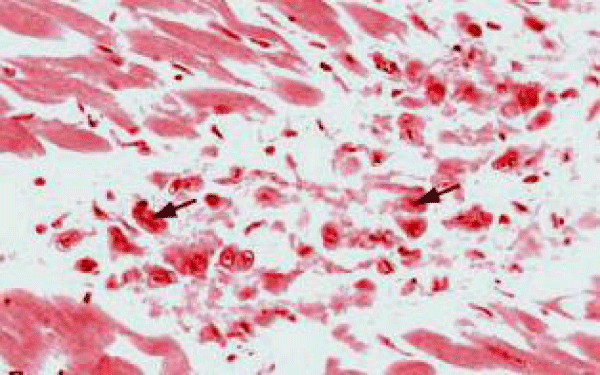
Figure 10: Reumatic Cardiopathy.
Involved in pathology related some endogenous products iper-production can be: Lisosomial pathology (rare disease), Platelet iperactivations, Thromboembolic unbalances in some cardiovascular condition, Trauma es myoglobin iper-production with renal damage (external moves), Pancreatic acute and cronic disease (high flogosis) by alcohol (external cause) or by cancer. Coma by iperammoniemia in example due by some severe hepatic disease. IRA and end stage renal pathology with accumulation of urea. This are only few example but we can observe many other examples that imply an esogenous or endogenous toxic substantia from Metabolism or catabolism or from other process. (immunomediated, oxidative and so on). Some Metal metabolism disorders: Levels of trace metals in the blood are controlled by special proteins. Inherited metabolic disorders can result in protein malfunction and toxic accumulation of metal in the body: Wilson disease (toxic copper levels accumulate in the liver, brain, and other organs). Hemochromatosis (excessive iron accumulation, which builds up in the liver, pancreas, joints, and heart, causing damage).
In pathologic disorder like: Urea cycle disorders; ornithine transcarbamylase deficiency and citrullinemia and other Inherited Metabolic Disorders. In all this situation we can think a toxicological mechanism: also an endogenous poison substantia or movens and related substrate. (Primary products or secondary to other external phenomena). Can we use better depurative methods or antidotic strategy in this situation? In order to better understand the concept is useful also to consider the cancer pathology: The characteristic metastatic process pathway: Why is possible to see a tendency of the migration towards certain organs rather than others. Why we see a tendency of migration tours this location compared to the other location when we are dealing with cancer metastasis? Why does the metastatic cell preferentially migrate to this specific location and it doesn’t touch other locations? If you have the same type of cells or similar, then why migration often happens in specific locations, and this is happening often not just one time. Is it possible to think in a multifactorial event, in which for instance the blood flow con play a role in one location compared to the other organs or tissues?
The secondary organ play an active role in this process? And the congestion process what role play in this game? Of course this could be combined with other physical or specific receptor profile or cellular mechanistic–physical factors, controlled by endogenous local Environmental mechanisms. Is it possible that we have some sort of dynamic or kinetic scenario that plays role at least partially in the specific location of migration? Of course we behave there are also some sort of intelligent migration scenarios rather than over simplistic Physical filtration Theory, in which body behaves as simple pipes death pipes. We Believe the body is not a house Plumbing to be influenced only by physical factors like filtration and that’s simple physical filtration would lead the selectivity in the body could act as some sort of incubator, for example some sort of fusion between two cells these are possibilities we are just posing possibilities. We are just portraying scenarios possible scenarios not necessarily concrete scenarios. Another relevant question is why in primary cancers, when we have for example different lobes, why with equal anatomical conditions or most likely equal vasculature or as we assume equal vasculature, we observe often first only one lobe getting cancer and the other lobes are not affected and this happens frequently on a pattern scheme? Is it possible or could it be that there is a difference in blood flow in different lobes or when one lobe is affected that specific lobe is stopping other lobes or making other lobes having less resources to develop cancer? Why if human bowel is about 7 metros long often cancer appears in one single site before?
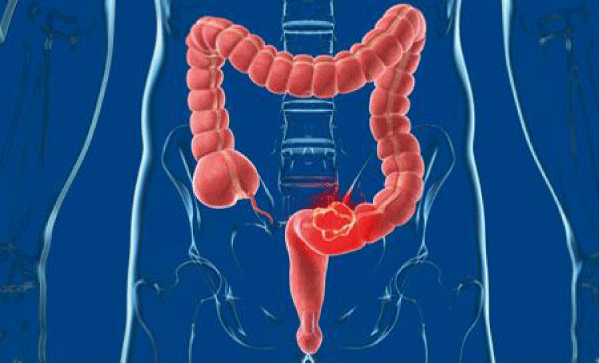
Figure 11: Bowel Cancer.
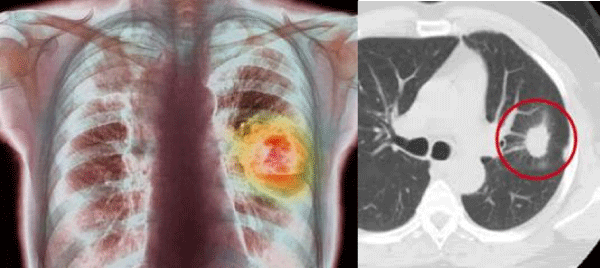
Figure 12: Lung Cancer.
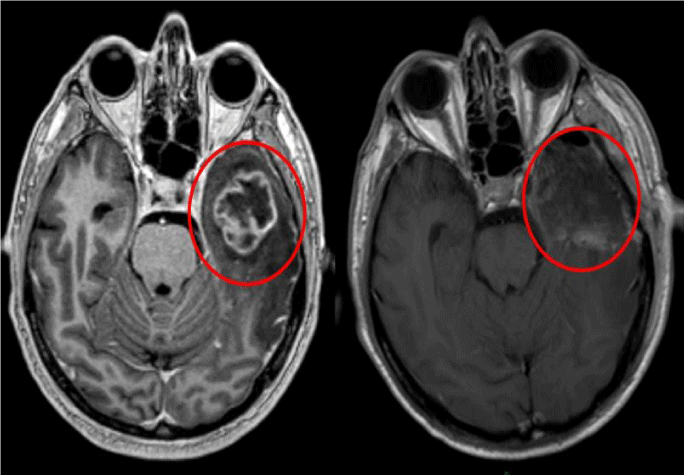
Figure 13: Brain Cancer.
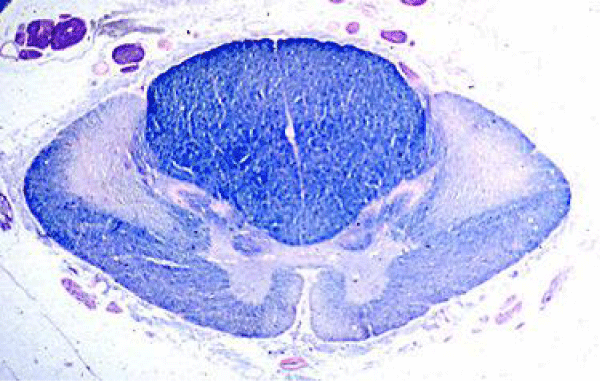
Figure 14: ALS. Degeneration of the corticospinal tracts Myelin stain.
So can we think to a MICROENVIRONMENTAL FACTORS to be added to the single genetic mutation profile to explain some Cancer disease presentations? (Figures 11-14). Could it be or maybe it is that there is some sort of congestion actor that makes predominantly one lobe affected first? (In example all pulmonary cell present the same probability to evolve in cancer in the different lobes). We have to also consider that cancer doesn’t have one type or cause and when we see one pattern or scheme happening in all cases and in different organs we are looking for wider answers. Then there is and maybe more important question and that is why the cardiovascular or hemato-vasculature factor really exercises such Sharp and important impact in some disease. Other example can be the coronaric disease, or atherosclerotic pathology that prefentially interest in example the vessel biforcation (by reologic factors). In this kind of process we can see that different factors influence the disease: high blood pressure, cholesterol level, fatty acid, platelet aggregation, lipo-peroxidation and other. This approach can be considered a sort of a sudden (or cronical) endogenus poison like condition. We should not forget that of course this is not only in lung cancer, we see the same type of behavior also in brain tumor, we see similar pattern in intestinal cancer and other.
Is really interesting to observe also some cancer development topography: in example human bowel is:
Normally about 7 metros long bust some cancer start from a single site: why? Is only due by a mutation? And why if the probability is the same in all bowel it start from a determinate zone?
The Why in example pulmonary cancer start often in only one lobe first? Certain physiological other factors are temporarily present in specific part of the body that can increase this probability? An endogenous local toxic microenvinoment time related? Observing certain natural processes you can notice that certain pathological conditions can be initiated or started from certain anatomically localized parts of the body ( topographic relationship ) and can cause certain disadvantages temporarily in that part of the body and only then maybe spread to other parts of the body. For instance you can consider in examples dental caries starts initially in certain specific teeth where there is an accumulation of bacteria and start to erode that specific tooth which depending on the extension and degree of that process may or may not be limited to that specific tooth or maybe only later start that as a nest for the other adjacent teeth. Dental carries can produce heart valvlepatie by lead into vessel of microbs that can affect cardiac valve. Another example is the blockade of certain arteries where it hits certain locations such a specifically where the arteries bifurcate where we have a sudden decrease of diameter while we have higher load of the blood which causes the deposit of certain metabolical chemicals, however in cases we don’t observe this deposit happening on both branches of this bifurcation but prevalently we observe one branch being affected but maybe only later the other branch would have some sort of the process but important is that this happens first in certain anatomical or microanatomical location, which means we have a process happening with a localized actor. (coronaropaty, stroke).
In this cases atherosclerotic disease related endogenous esogenous lipid profile, platelet iperactivation, genetic profile (pro-coagulant factors espression). Also in other scientific field as geological and related sciences is observed that where forces modules acts together often some phenomena start preferentially in a determinate site giving a general global effect. We can see that in example in old wall first appears broken lines and then all the wall fall down. Are this only stochastic event? Or other factor contribute to the final exitus? (But in a wall collapse also if trying to repair a crack often not prevent the global final effect).
Materials and Methods
With an observational approach and using PUBMED database various articles are analysed to verify the global movens involved in some pathological condition (like cancer) useful to produce new therapeutic strategy to improve the patient’s clinical outcomes.
Experimental project
In order to experimentally verify endogenous toxicological effect HYPOTESYS in some pathology is possible to think to an in vitro condition: Tissue interested by a determinate pathological event + the same local endogenous environmental substancies. Tissue interested by pathological event+ other local endogenous environmental substancies (not by the same tissue origin). Tissue not interested in pathological event+other local endogenous environemental substancies (from tissue affected). Tissue not interested in ptaholofical effect + other local endogenous enviromenetal substanties from tissue not affected). In this way is possible to verify the effect of local endogenous environment in progression of a determinate pathological condition in example using depurative strategy or other to reduce concentration of endogenous substanties involved in the pathological process. In this kind of project is possible to test different strategies like: diagnostic, preventive, detoxicant, antidotic and other: Reduce syntetic process of endogenous toxic molecule of movens increase this catabolic process of the endogenous toxic molecule inactivate this subtancties, Remove the toxic substanties, Accelerate elimination, Reduce complexive time of actions, Use of an antidothe remedy, Use a depurative strategy.
A new diagnostic system usefull to detect early topographic modify that can contribute to the endogenous toxicology process. (Imaging, nuclear medicine, molecular biology, biochemistry tests, kinetics and other).
Results
From literature
Lakatos et al., writed “Our recommandation: all newborns should be screened for ASD.
Particularly the premature babies and infants suffering from hyperbilirubinemia. These conditions significantly increases the prevalence of NDs, including ASD” [1].
Luisetto writed that: ”Concepts as toxical doses, time of exposition, cumulative dosage, kinetics, dynamics, methabolism Iatrogenic ADME and other toxicological parameter can be usefully introduced also in neuro-immune toxicology to adeguately focus a physio-pathogenetic phenomena. The results related to the references citated show a specific effect of a systemic drugs in a local place as brain. We think that observing a specific side effect of a drug can be a right method to clear some interference between immunologic status and some development disorder” [2].
According to article minset kinetics:”Can we compare the mindset kinetics to other methabolic kinetics? Are really so different this aspects? [3]. “Can we think to a sort of saturate condition in some situation? Can we think to a maximal velocity in management of simultaneous or high stressant stimulus?” [3].
Maniscalco et al., showed that: “Atherosclerosis is a complex process with multiple mechanisms and factors contributing to its initiation and progression. Detection and quantification of coronary artery calcium (CAC) scores with electron beam tomography has been shown to correlate with obstructive and non-obstructive coronary artery disease (CAD). Pathogen-triggered calcification could play a role in CAD. Recent reports suggest that infectious blood Nano bacteria (NB) emerge to be such a trigger” [4].
Toxics. 2014; 2(1): 17-34. Chemical Atherogenesis: Role of Endogenous and Exogenous Poisons in Disease Development.Ross MK1, Matthews AT1, Mangum LC1. “Chemical atherogenesis is an emerging field that describes how environmental pollutants and endogenous toxins perturb critical pathways that regulate lipid metabolism and inflammation, thus injuring cells found within the vessel wall. Despite growing awareness of the role of environmental pollutants in the development of cardiovascular disease, the field of chemical atherogenesis can broadly include both exogenous and endogenous poisons and the study of molecular, biochemical, and cellular pathways that become dysregulated during atherosclerosis. This integrated approach is logical because exogenous and endogenous toxins often share the same mechanism of toxicity. Chemical atherogenesis is a truly integrative discipline because it incorporates concepts from several different fields, including biochemistry, chemical biology, pharmacology, and toxicology. This review will provide an overview of this emerging research area, focusing on cellular and animal models of disease” [5].
Hyperglycemia, oxidative stress, and vascular disease “Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part I. The alterations in vascular homeostasis due to endothelial and smooth muscle cell dysfunction are the main features of diabetic vasculopathy favouring a pro-inflammatory/thrombotic state which ultimately leads to atherothrombosis. Macro- and microvascular diabetic complications are mainly due to prolonged exposure to hyperglycemia clustering with other risk factors such as arterial hypertension, dyslipidemia as well as genetic susceptibility. Interestingly, nephropathy, retinopathy, and diabetic vascular disease are in line with the notion that endothelial, mesangial, and retinal cells are all equipped to handle high sugar levels when compared with other cell types. The detrimental effects of glucose already occur with glycemic levels below the threshold for the diagnosis of diabetes. This is explained by the concept of ‘glycemic continuum’ across the spectrum of prediabetes, diabetes, and cardiovascular risk. 5–8 early disglycemia caused by obesity-related insulin resistance or impaired insulin secretion is responsible for functional and structural alterations of the vessel wall culminating with diabetic vascular complications. The initial trigger whereby high glucose concentrations alter vascular function is the imbalance between nitric oxide (NO) bioavailability and accumulation of reactive oxygen species (ROS), leading to endothelial dysfunction. Hyperglycemia-induced generation of superoxide anion (O2−) inactivates NO to form peroxynitrite (ONOO−), a powerful oxidant which easily penetrates across phospholipid membranes and induces substrate nitration. Protein nitrosylation blunts activity of antioxidant enzymes and endothelial NO synthase (eNOS). Importantly, reduced NO bioavailability is a strong predictor of cardiovascular outcomes.
Mechanisms of hyperglycemia-induced vascular damage. High intracellular glucose concentrations lead to PKC activation and subsequent ROS production by NADPH oxidase and p66Shc adaptor protein. Increased oxidative stress rapidly inactivates NO leading. Overproduction of ROS by mitochondria is considered as a causal link between elevated glucose and the major biochemical pathways involved in the development of vascular complications of diabetes. Indeed, hyperglycemia-induced ROS production triggers several cellular mechanisms including polyol and hexosamine flux, advanced glycation end products (AGEs), protein kinase C (PKC) activation, and NF-kB-mediated vascular inflammation. One of the main sources of ROS in the setting of hyperglycemia is represented by PKC and its downstream targets. The hyperglycemic environment induces a chronic elevation of diacyglycerol levels in endothelial cells with subsequent membrane translocation of conventional (α, β1, β2) and non-conventional (δ) PKC isoforms. Once activated, PKC is responsible for different structural and functional changes in the vasculature including alterations in cellular permeability, inflammation, angiogenesis, cell growth, extracellular matrix expansion, and apoptosis. An important consequence of PKC activation is ROS generation. In vascular endothelial cells, hyperglycemia-induced activation of PKC increases superoxide production via NADPH oxidas. Indeed, treatment with a PKCβ inhibitor suppresses NADPH-dependent ROS generation.
It has been reported that glucose-induced activation of PKC β2 isoform phosphorylates p66Shc at serine 36 leading to its translocation to the mitochondria, cytochrome c oxidation and accumulation of ROS into the organelle. The p66Shc adaptor protein functions as a redox enzyme implicated in mitochondrial ROS generation and translation of oxidative signals into apoptosis. Interestingly, diabetic p66Shc−/− mice are protected against hyperglycemia-induced endothelial dysfunction and oxidative stress. PKC affects NO availability not only via intracellular accumulation of ROS but also by decreasing eNOS activity. PKC also leads to increased production of endothelin-1 (ET-1) favouring vasoconstriction and platelet aggregation. The role of ET-1 in the pathophysiology of diabetic complications is confirmed by the observation that the activity of endogenous ET-1 on ET (A) receptors is enhanced in the resistance vessels of patients with diabetes. In the vessel wall, PKC-dependent ROS production also participates in the atherosclerotic process by triggering vascular inflammation. Indeed, ROS lead to up-regulation and nuclear translocation of NF-kB subunit p65 and, hence, transcription of pro-inflammatory genes encoding for monocyte chemoattractant protein-1 (MCP-1), selections, vascular cell adhesion molecule-1 (VCAM-1), and intracellular cell adhesion molecule-1 (ICAM-1). This latter event facilitates adhesion of monocytes to the vascular endothelium, rolling, and diapedesis in the sub-endothelium with subsequent formation of foam cells. Secretion of IL-1 and TNF-α from active macrophages maintains up-regulation of adhesion molecules by enhancing NF-kB signalling in the endothelium and also promotes smooth muscle cells growth and proliferation, inhibition of PKC β2 isoform blunts VCAM-1 up-regulation in human endothelial cells upon glucose exposure.
Endothelial dysfunction in diabetes is not only the result of impaired NO availability but also of increased synthesis of vasocontrictors and prostanoids. PKC-mediated cyclooxygenase-2 (COX-2) up-regulation is associated with an increase of thromboxane A2 and a reduction of prostacyclin (PGI2) release). These findings suggest that PKC is the upstream signaling molecule affecting vascular homeostasis in the setting of hyperglycemia. Mitochondrial ROS also increase intracellular levels of the glucose metabolite methylglyoxal and AGEs synthesis. In experimental diabetes, methylglyoxal is a key player in the pathophysiology of diabetic complications through oxidative stress, AGEs accumulation, and endothelial dysfunction. Generation of AGEs leads to cellular dysfunction by eliciting activation of the AGEs receptor (RAGE). AGE-RAGE signaling in turn activates ROS-sensitive biochemical pathways such as the hexosamine flux. In the hyperglycemic environment, an increased flux of fructose-6-phosphate activates a cascade of events resulting in different Glycosilation Patterns which are responsible for deregulation of enzymes involved in vascular homeostasis. O-GlcNAcylation at the Akt site of eNOS protein leads to reduced eNOS activity and endothelial dysfunction. Glycosylation of transcription factors causes up-regulation of inflammatory (TGFα, TGFβ1) and pro-thrombotic genes (plasminogen activator inhibitor-1 Glucose induced-ROS production also activates the polyol pathway flux involved in vascular redox stress. Accordingly, hyperactivation of this pathway has been associated with increased atherosclerotic lesions in diabetic mice” [6].
According Luisetto M, Mashori GR, Nili-Ahmadabadi B, Khan FA, Khan KR. Mindset kinetics and some depression status: A new quantitative model under biochemical - toxicology approach?
Insights Depress Anxiety. 2019; 2: 029-039. “Considering the stressant stimolus like an endogenous- exogenous toxic condition factor can be interesting to think to new kind of Remedies.A Toxicology status can be considered also a overuse of a system that can producegreat unbalances in physiology in some apparatus. A Toxicology status can be considered also an overuse of a system that can produce great unbalances in physiology in some apparatus” [7].
Luisetto M, Naseer A, Ghulam R M, Ahmed Y R, Farhan A K,et al. Endogenous Archeological Sciences: Anatomy, Physiology, Neuroscience, Biochemistry, Immunology, Pharmacology, Oncology, Genetics as Instrument for A New Field of Investigation? “Residual organs, genes, metabolic pathways, immune response, ancestral systems can be observed in actual human being as an archeological ruins to testify an evolutive process. Emotional control, fear, aggressivity, sexual and surviving instinct, some immune process, onco suppressor and and many other Functions are strictly related with a common evolution and with real objectivable evidence” [8].
Mechanisms involved in breast cancer liver metastasis. Rui Ma, Yili Feng, Shuang Lin, Jiang Chen, Hui Lin, Xiao Liang, Heming Zheng, and Xiujun Cai corresponding author “Hypoxia-inducible factor-regulated genes “Hypoxia-inducible factors (HIFs) activate the transcription of target genes that are involved in many aspects of breast cancer progression, such as angiogenesis, metabolic reprogramming, local tissue invasion, and metastasis . It has been reported that HIFs not only activate lysyl oxidase (LOX) directly to inhibit liver metastases, but osteopontin (OPN), vascular endothelial growth factor (VEGF), and TWIST promote BCLM. It has been suggested that some of the hypoxia-inducible factor-regulated genes contribute to BCLM” [9].
Lysyl oxidase is essential for hypoxia-induced metastasis. Erler JT1, Bennewith KL, Nicolau M, Dornhöfer N, Kong C, Le QT, Chi JT, Jeffrey SS, Giaccia AJ. “Metastasis is a multistep process responsible for most cancer deaths, and it can be influenced by both the immediate microenvironment (cell-cell or cell-matrix interactions) and the extended tumour microenvironment (for example vascularization). Hypoxia (low oxygen) is clinically associated with metastasis and poor patient outcome, although the underlying processes remain unclear. Microarray studies have shown the expression of lysyl oxidase (LOX) to be elevated in hypoxic human tumour cells. Paradoxically, LOX expression is associated with both tumour suppression and tumour progression, and its role in tumorigenesis seems dependent on cellular location, cell type and transformation status. Here we show that LOX expression is regulated by hypoxia-inducible factor (HIF) and is associated with hypoxia in human breast and head and neck tumours. Patients with high LOX-expressing tumours have poor distant metastasis-free and overall survivals. Inhibition of LOX eliminates metastasis in mice with orthotopically grown breast cancer tumours. Mechanistically, secreted LOX is responsible for the invasive properties of hypoxic human cancer cells through focal adhesion kinase activity and cell to matrix adhesion. Furthermore, LOX may be required to create a niche permissive for metastatic growth. Our findings indicate that LOX is essential for hypoxia-induced metastasis and is a good therapeutic target for preventing and treating metastases” [1].
Endogenous and exogenous factors in carcinogenesis: limits to cancer prevention
Werner K, Lutz T. Fekete “Organ-specific cancer incidence rates can vary dramatically between low- and high-incidence areas. Such differences are due to heritable susceptibility determinants, risk factors associated with the environmental and local living conditions (e.g., viruses, pollution), and personal life-style factors. For organs showing large differences between cancer registries, exogenous factors might be most important, while for organs showing only small differences, endogenous and unavoidable factors are expected to be more important. In this work, a working hypothesis based on descriptive cancer epidemiology is presented to estimate, in a quantitative manner, the unavoidable contribution to the process of carcinogenesis and to discuss limitations to individual cancer prevention. Cumulative cancer incidence rates for a 75-year period of life (CR74, in percent) were taken from IARC Scientific Publication No. 120 (1992). For each organ, values were ranked in ascending order, and the ratio between high-rate and low-rate registries (90th percentile/10th percentile) was determined. This measure of variability among registries differed strongly between organs. Largest ratios were seen for organs with well-known exogenous risk factors, such as pharynx, lip, tongue, mouth, liver, esophagus, and melanoma in males, and lung, esophagus, gallbladder, liver, and bladder in females. Small ratios were seen for rectum, brain, colon, and Hodgkin’s disease in males, and breast, rectum, ovary, brain, and colon in females. It is concluded that the process of carcinogenesis in the latter organs has a stronger endogenous/unavoidable component, for some tissues possibly of hormonal type. A fictitious population was composed where, for each organ, the minimum reported cancer rate was taken. When based on all cancer registries world-wide, CR74 sums over all sites of 2.0% and 2.3% resulted in males and females, respectively. When only Central/Western European countries were included in the analysis in order to reduce differences in risk factors nos, 1 and 2, the sum of the minimum values was 10.4% and 8.7%. After correction of the data for smoking, ‘minimum’ cancer incidence rates in males and females were estimated to be 7.6% and 6.8%. Based on a median cancer incidence rate for nonsmoking males in Europe of about 21%, therefore, individual preventive measures taken by a nonsmoker can reduce the cancer risk, on average, ‘only’ by a factor of about 3. A considerable fraction of cases thus appears to be hardly avoidable“[11].
“We start our paper observing that in past centuries physicians in some cardiologic disease were used to prescribe to the patient to take a long rest in order to recuperate their health status. In past centuries it wasn’t available high efficient drugs strategies and so to take a long rest without physical and psychological stress contributes to this process. Also in oriental medicine we can see body balances strategies, and also in some psycoaanalitc techniques we can see that time is relevant to re-equilibrate some conditions (in example acute stress). We can think that the main factors involved are TIME and LONG REST in order to balance the physiologic functions. In some case it was observed complete resolve in some situations. In example we can think that a metabolic unbalances can create this situation and the time make possible to restore. In toxicology usually are high considered the external environmental factors but we think we must observe under toxicological methods also the inside intra-extra cellular local microenvironment (paraphysiologic-pathologic conditions). In some pathology the time is relevant added to local micro environment and inters cellular communication situations. We must consider an intra- local toxicology aspect time related to better verify some pathologic process under a new light. In some time related local metabolic-catabolic-toxic status we can observe some cellular effect resulting in some organ failure. The time involved in resolve some temporary gradients or the velocity involved in this process can be fundamental. The same effect related to too much rapid evolution or too slow reduction in balancing equilibrates physiologic systems.(The same the reduced effect showed in example in sports trained in SCD vs not trained activate platelet in trigger coronary artery spams, amygdala temporal iper activation or other examples).
We need to introduce more toxicological methods in some pathologies in order to clear some relevant aspect in etiology, diagnosis and therapy” [12]. “Can we think some endogenus toxicologic movens in some heart pathologies? Mathabolic catabolic Kinetics is relevant factor in balancing some cellular- tissue responces? Some Endogenus gradients time related can be responsible in some organ failure? In toxicology field usually are high considered the external environmental factors as iatrogenic substantia but we think we must observe under toxicological methods also the endogenus intra-extra cellular local microenvironment (in paraphysiologic-pathologic situations). In some cardio vascular pathology the time is relevant added to endogenus local micro environment and inters cellular communication status. We must consider an endogenus intra-local toxicology aspect time related to better verify some pathologic process under a new light. In some time related cardiovascular local metabolic-catabolic-toxic status we can observe some cellular effect resulting in global organ failure. The time involved and kinetics aspect in resolve some temporary methabolic-catabolic gradients or the velocity involved in this process can be fundamental. The same effect related to too much rapid evolution or too slow reduction (kinetics) in balancing equilibrates some physiologic systems” [13].
James A Swenberg et al. writed that: “Going beyond chemicals that form identical endogenous and exogenous DNA adducts, there are approximately 50,000 endogenous DNA lesions in every living cell. This steady- state amount of DNA damage has long been considered to represent a major source of cancer and other diseases. Despite this, it has not been taken into consideration in risk assessments in determining what exposures actually produce disease. For that matter, epidemiology has not adequately utilized information on biomarkers to assist in the de- termination of causality. Such data can help support or refute causal associations. We propose that this approach is set in an embryonic state of knowledge but strongly believe that public health and effective regulation of chemicals will be strengthened by science-based determinations of causality and promulgations of risk. To achieve this, we must have better data on low-dose mutagenicity, improved mode of Action understanding that covers high- to low-dose ranges, and species differences and similarities. We can then move forward, embracing public health protective actions that are based on science. This includes the application of reasonable additional factors for susceptible individuals” [14].
Sim BK et al: “Considerable progress has been made in the understanding of the molecular structure and mechanistic aspects of Angiostatin and Endostatin, endogenous angiogenesis inhibitors that have been shown to regress tumors in murine models. The growing body of literature surrounding these molecules and on the efficacy of these proteins is in part due to the ability to generate these proteins in recombinant systems as well characterized molecules. Recombinant human Angiostatin and Endostatin are in Phase I trials, following the manufacture of clinical grade material at large scale. This review highlights the recent advances made on understanding the structure and function of Angiostatin and Endostatin” [15].
According Emily R, Finch et al: “Supplementation with nontoxic doses of micronutrient selenium has been shown to alleviate chronic myelogenous leukemia (CML) via the elimination of leukemia stem cells (LSCs) in mice. This treatment provides a new and novel method for eliminating the LSCs that are otherwise not targeted by existing therapies. The antileukemic effect of selenium was dependent on the production of endogenous cyclopentenone prostaglandins (CyPGs), Δ-12 prostaglandin J2 (Δ12-PGJ2), and 15-deoxy-Δ12, 14-prostaglandin J2 (15d-PGJ2). Here, we show that these endogenous CyPGs, produced by mice maintained on selenium-supplemented diets, alleviate the symptoms of CML through their ability to activate the nuclear hormone receptor, peroxisome proliferator activated receptor γ (PPARγ). GW9662, a potent PPARγ antagonist, blocked the antileukemic effect of selenium supplementation by significantly reducing CyPGs. This effect was mediated by an increase in 15-prostaglandin dehydrogenase (15-Pgdh) activity, which oxidizes and inactivates Δ12-PGJ2 and 15d-PGJ2. In contrast, treatment with the PPARγ agonist pioglitazone mimicked selenium supplementation. This treatment led to decreased 15-Pgdh activity and increased CyPG levels, which inhibited CML progression. Selenium-dependent activation of PPARγ mediated by endogenous CyPGs decreased Stat5 expression leading to the downregulation of Cited2, a master regulator of LSC quiescence. These studies suggest a potential role for selenium supplementation as an adjuvant therapy in CML” [16].
Annonacin, a natural mitochondrial complex I inhibitor, causes tau pathology in cultured neurons. Escobar-Khondiker M1, Höllerhage M, Muriel MP, Champy P, Bach A, Depienne C, Respondek G, Yamada ES, Lannuzel A, Yagi T, Hirsch EC, Oertel WH, Jacob R, Michel PP, Ruberg M, Höglinger GU.
“A neurodegenerative tauopathy endemic to the Caribbean island of Guadeloupe has been associated with the consumption of anonaceous plants that contain acetogenins, potent lipophilic inhibitors of complex I of the mitochondrial respiratory chain. To test the hypothesis that annonacin, a prototypical acetogenin, contributes to the etiology of the disease, we investigated whether annonacin affects the cellular distribution of the protein tau. In primary cultures of rat striatal neurons treated for 48 h with annonacin, there was a concentration-dependent decrease in ATP levels, a redistribution of tau from the axons to the cell body, and cell death. Annonacin induced the retrograde transport of mitochondria, some of which had tau attached to their outer membrane. Taxol, a drug that displaces tau from microtubules, prevented the somatic redistribution of both mitochondria and tau but not cell death. Antioxidants, which scavenged the reactive oxygen species produced by complex I inhibition, did not affect either the redistribution of tau or cell death. Both were prevented, however, by forced expression of the NDI1 nicotinamide adenine dinucleotide (NADH)-quinone-oxidoreductase of Saccharomyces cerevisiae, which can restore NADH oxidation in complex I-deficient mammalian cells and stimulation of energy production via anaerobic glycolysis. Consistently, other ATP-depleting neurotoxins (1-methyl-4-phenylpyridinium, 3-nitropropionic, and carbonyl cyanide m-chlorophenylhydrazone) reproduced the somatic redistribution of tau, whereas toxins that did not decrease ATP levels did not cause the redistribution of tau. Therefore, the annonacin-induced ATP depletion causes the retrograde transport of mitochondria to the cell soma and induces changes in the intracellular distribution of tau in a way that shares characteristics with some neurodegenerative diseases” [17].
Jing Xu, et al: “The International Agency for Research on Cancer classifies hexavalent chromium (Cr (VI)) as a human carcinogen. As reported, cancer mortality was higher in Cr(VI)-contaminated areas. We conducted a cross-sectional study in rural areas of north-eastern China. Malondialdehyde (MDA), glutathione peroxidase (GSH-Px), superoxide dismutase (SOD) and catalase (CAT) were used as oxidative stress parameters, and 8-hydroxy-2 deoxyguanosine (8-OHdG) as a DNA damage biomarker. We collected information on demographics, lifestyles and length of residence from all participants using a questionnaire. Biological specimens and environmental media samples were collected on the same day as the survey was done. We used t-test, χ2 test, Wilcoxon rank-sum test and multivariate linear regression analysis. The study included 319 participants exposed to Cr (VI) and 307 unexposed participants, with 447 women and 179 men. These participants met the following criteria: (1) living in the areas for more than 10 years; (2) age older than 18 years; and (3) without occupational chromium exposure. Our study revealed that serum concentration of MDA (p<0.001), serum activities of CAT (p<0.001) and GSH-Px (p<0.001), as well as urine concentration of 8-OHdG (p=0.008) in the exposed group were significantly higher than those in the unexposed group. However, serum SOD activity was significantly lower in the exposed group, compared with that in the unexposed group (p<0.001). Cr (VI) exposure and smoking have an interaction effect on GSH-Px activity (p<0.05). Cr (VI) exposure and alcohol drinking also have an interaction effect on GSH-Px activity (p<0.05). Longer residence in the exposed areas increased the oxidative levels (p<0.05).The findings of this study showed elevated oxidative stress and DNA damage in people exposed to Cr (VI)” [18].
Luisetto et al. in 2019 writed: “According all this scientific literature is possible to conclude that: In those biologic systems we have given as models, many of biological processes go through a first phase to a final phases which in some cases transitions to a more advantageous, or a sort of parasitism- simbiontic process with advantages to all or what we call it win -win mutual benefits situation (organism and parassites). Once we examine all these models, who would extrapolate a similar model for metastasis which we call it the “seed and soil” hypothesis: we have different role played by dissemination process of metastatic cells and the secondary organ role. In order to hypothesize and develop new ideas of innovative therapeutic strategies in order to stop, control or the least delay metatstatic process, it is relevant to verify the role played by the secondary organ in boosting metastatic cells inside. And it’s not anymore just an entrapment passive role but we think the evidence shows that there must be active role. So by examining all those evidence, it is incumbent upon us to establish that a simple passive filtration process and interaction are not sufficient to explain many episodes we see and there must be some sort of tissue and organ properties (such as high metabolism, high turnover, high oxygen, availability or some sort of involvement of the immune systems) that could take part in this. What we are suggesting is that there must be something more than passive filtration, there must be an active role in growth vs other organ without this characteristics. Could it bethat the metastasis uses a parasite-like – simbiontic exchange? And what could be theconsequences in the strategies taken in new treatments?” [19].
Schwartz CJ et al: “Atherosclerosis is conceptually defined as the result of a multiplicity of interactive cascades among injurious stimuli and the healing responses of the arterial wall, occurring concurrently within a hyperlipidemic environment. In this discussion, the inflammatory nature of the disease is emphasized. Four aspects of the pathophysiology of atherogenesis are addressed: (1) The role(s) of fluid mechanical or hemodynamic stresses in the focal initiation and/or augmentation of lesions is discussed in terms of the influence of shear stress on endothelial cellular geometry, compliance, membrane anisotropy (r), low-density lipoprotein (LDL)-receptor expression, intracellular potential and replication; (2) mechanisms of blood monocyte recruitment to the arterial intima, including the roles of chemoattractants such as smooth muscle cell-derived chemotactic factor and oxidized LDL; (3) the alternate or “scavenger” receptor pathway of the macrophage and its pivotal roles in foam cell formation and plaque pathogenesis; and (4) the emerging significance of various lipoprotein modifications, and in particular, the oxidative modification of LDL, which facilitates the uptake of the cytotoxic oxidized LDL via the scavenger receptor, thus providing a non-down-regulating mechanism for foam cell formation and plaque development. Evidence indicates that the antioxidant drug probucol prevents the oxidative modification of LDL, thereby retarding atherogenesis independently of cholesterol reduction” [20].
Mogoantă SS et al: “Colorectal cancer (CRC) is one of the most common and most serious malignancies worldwide. Its incidence has increased by more than 200000 in 2008, both in men and in women. Although CRC is a well-studied malignancy which has a slow progression, known risk factors and pre-neoplastic lesions that can be detected and treated, its incidence is on the rise. In our study, we clinically, histologically and immunohistochemically evaluated a group of 317 patients with colorectal cancer who underwent surgery. The trial included 317 colorectal cancer patients hospitalized in the second Department of General Surgery within the Emergency County Hospital of Craiova, Romania, between January 2005 and December 2009, aged between 18 and 89 years. After undergoing clinical and laboratory work-up, all patients were submitted to surgery with curative intent. Resection specimens were collected and histological slides were produced from the biological material. Usual histological staining, Hematoxylin-Eosin and trichromic Goldner-Szekely, as well as immunohistochemistry with anti-Ki67, anti-caspase 3 and anti-p53 and anti E-cadherin antibodies was also performed. Regarding gender distribution of cases in the study group was a slightly higher incidence in the number of women affected by neoplasia (n=166, 52.35%) than males (n=151, 47.65%). Analysis of incidence per decade of age showed highest Figures between 61-70 years, but we also observed comparable values for the decade 51-60 years. Analysis of topography showed higher incidence of cancer of the rectum (119 cases, representing 37.53%) compared to individual segments of the colon. Average size determined for all locations was 5.05 cm, with a median located at 4.82 and a standard deviation of 1.99. Regarding the degree of cell differentiation, out of the total of 245 adenocarcinomas, a number of 87 (35.52%) were well-differentiated adenocarcinomas, 127 (51.83%) were moderately differentiated, and 31 (12.65%) cases were poorly differentiated adenocarcinomas. Index of cell proliferation, Ki67, had a moderate and intense reaction to all the cases studied. Very few tumor cells were immunohistochemically positive for caspase 3, regardless of the degree of tumor differentiation. E-cadherin was intense in well-differentiated adenocarcinomas. In our study, of 42 colon adenocarcinomas, 29 (69%) were highly positive to anti-p53 antibody, the remaining being negative. Colorectal cancer was diagnosed especially in people over 50 years.. More than half were presented in stages III and IV. The histopathological study showed that about 98% of colorectal neoplasms were adenocarcinomas, frequently with moderate differentiation” [21].
Manish K Thakur et al: “The risk for development of a second primary lung cancer (SPLC) after treatment of an initial primary lung cancer (IPLC) is around 1% to 2% per patient per year. The present screening and surveillance guidelines do not adequately address this particular patient population” (22). According to the article “Surgery and new Pharmacological strategy in some atherosclerotic chronic and acute conditions 2017: “Related to the bibliography reported and other in biomedical database available today. We have seen that in many situation pharmacological molecules are added to other substrate in order to improve the effect in local site, reducing global side effect. The same we have seen that some interventional radiology techniques have been used to avoid general classic surgery with good clinical results as we can see in biomedical databases and scientific library. Observing the composition of calcified aortic valves we can think that a new system that can be able to dissolve the salt precipitation can be used to improve the valve phisiology versus a complex classic surgery. Is universally known that the patient health highly is involved in artery phisio-pathology and that cardiovascular disease are responsible of a great number of preventable exitus. Using the association of interventistic radiology strategy to inject in valve tissue a mixture of pharmacological agent (complexant or other) with a delivery system designed to improve the time of action in site we can think to obtain an relevant effect to be considered (starting from animal models). So we can search a strategy systems to make possible the pharmacological molecules can arrive in the Site interested by the pathology avoiding the global toxicology of some drugs (as EDTA). In example we can see that commonly surgery is used in aortic valvle disease in order to prevent CHF and re modulations of cardiac tissue. This imply a complex surgery situation and to find other solution can be an interesting option. We have seen that vascular calcification is heavly involved in atherosclerotic disease and that this phenomena can be better showed also by tomography and RAMAN SPECTROSCOPY. And that using innovative drugs delivery systems we can improve clinical effect reducing total toxicity. And even if the chelanting therapy is not accepted by scientific world [9], we must say that this could be related to a systemic sub ministration with global toxicity, and not related to local treatment. And we can see that avila et al write that TACT, the first large-scale trial of chelation therapy for atherosclerotic coronary disease, found that EDTA chelation therapy reduced the risk of a composite of adverse cardiovascular outcomes, particularly among patients with diabetes. Before disodium EDTA chelation can take its place among other accepted therapies in the routine care of post-MI patients, however, it is important that further replicative and mechanistic clinical trials be performed.
King SB et al: Different strategies can be applied in some coronaric disease with different profile of results and side effect: Coronary artery disease (CAD) is one manifestation of ischemic heart disease, which is the leading cause of mortality in the world. In addition to preventive medical therapy and lifestyle changes, consideration of revascularization of obstructed arteries to reduce ischemia, alleviate angina, and improve quality of life is a mainstay of current practice. However, the benefits of different methods of revascularization in particular patient populations are debated. Percutaneous coronary intervention (PCI), which involves placement of intracoronary stents in most patients, is a less invasive procedure than coronary artery bypass graft (CABG) surgery. Although it is generally accepted that patients with single-vessel obstructive CAD are best treated with PCI, patients with multivessel CAD have a higher ischemia burden, a greater risk for developing recurrent ischemic events, and a higher mortality. It is in this patient population where the debate over revascularization with stents versus surgery continues. In order to dissolve the atherosclerotic plaques precipitated on cardiac vales, what we can think to physical system, inject inside the vascular wall a mixture of a polymer-based extended the Release delivery system.
With a chelating agent will eat up the cationic precipitations if it is a sal such as calcium containing material.
Or we can use steroid agents if it is a cholesterol-based we can use a type of material that will soften the plaques because of the substitution of cholesterol with another sterole like sitosterol or other molecules with this kind of activities [24].
Sim BK et al: “Considerable progress has been made in the understanding of the molecular structure and mechanistic aspects of Angiostatin and Endostatin, endogenous angiogenesis inhibitors that have been shown to regress tumors in murine models. The growing body of literature surrounding these molecules and on the efficacy of these proteins is in part due to the ability to generate these proteins in recombinant systems as well characterized molecules. Recombinant human Angiostatin and Endostatin are in Phase I trials, following the manufacture of clinical grade material at large scale. This review highlights the recent advances made on understanding the structure and function of Angiostatin and Endostatin [26].
K Lutz et al: “In 1981, Doll and Peto published an epidemiological attempt to estimate the proportions of cancer deaths attributable to various factors (Doll and Peto 1981) Tobacco and diet each were found to contribute about one-third to the avoidable cancer mortality While this estimate was considered to be quite precise for tobacco, the range of 10 %-70 % for diet indicated the uncertainty for this factor. The authors also stated that no predominant dietary carcinogenic factor could be named Therefore, in terms of reliably established ways of avoiding cancer, only avoidance of tobacco (30%), alcohol (3%) and obesity (2%) represent practicable preventive measures (Peto 1985). This sobering analysis is supported by cancer mortality data in health-conscious groups such as Mormons: the age-adjusted cancer mortality of Californian Mormons was 66 % and 82 % of the rate reported for the average male and female U S white, respectively (Enstrom 1980). The reduction was almost exclusively due to tumors associated with cigarette smoking and alcohol consumption.
Nevertheless, the understanding prevails that cancer is a preventable disease if only we knew the relevant risk factors. Alternatively, a background rate of cancer formation might be unavoidable or even endogenous if this is the case, cancer prevention would have to focus also on possibilities to modulate the rate of the background process of malignant cell transformation. Transformation of a normal cell to a cancer cell requires multiple changes in genes involved in the control of cell division. The changes are passed on to the progeny, indicating the heritable aspect. The first chemicals to be recognized as carcinogens were later shown to damage DNA by covalent binding For this primary DNA lesion to be fixed as a heritable mutation, the DNA has to be replicated .The question about endogenous aspects of carcinogenesis therefore is primarily a question about endogenous DNA damage and constitutive aspects of tumor promotion, eg, cell division. In 1972, Lindahl and Nyberg showed that DNA is not entirely stable in aqueous solution Of the changes documented, depurination was the most frequent (Lindahl and Nyberg 1972) .This background DNA damage was an accepted factor for spontaneous mutagenesis but not for spontaneous cancer formation, probably because the mutation theory of carcinogenesis was not generally accepted at that time In addition, in view of efficient DNA repair processes, and in the absence of data on the steady-state level of DNA damage, the impression prevailed that, under normal conditions, all DNA damage can be repaired before DNA replication My statement expressed in 1982 ‘that a ground-level DNA damage is unavoidable,’ with the conclusion that “what is normally called spontaneous tumor incidence is partly due to this ‘constitutive’ DNA damage” (Lutz 1982) was heavily challenged.
The discussion of background DNA damage was stimulated when products of oxidative DNA damage were shown to be excreted in human urine (Cathcart et al.1984) Not much later, numerous DNA modifications were shown with the phosphorus-32 postlabeling method in untreated control animals (Randerath et al 1986) Reviews on endogenous genotoxic agents and processes followed (Ames and Gold 1991; Farmer et al 1993; Loeb 1989; Lutz 1990; Mamett and Burcham 1993; Randerath et al 1992; Wei and Samson 1993. The focus was on two groups of DNA-damaging agents, endogenous electrophiles such as aldehydes and S-adenosylmethionine, and reactive oxygen species. Today, the evidence of background DNA damage is so strong that spontaneous carcinogenesis has to be taken into consideration in all as- Two approaches can be envisaged to estimate the contribution of unavoidable genotoxicity in cancer induction. One involves measuring background levels of DNA damage and comparing it with the DNA damage resulting from high-level carcinogen exposure, such as cigarette smoking, certain workplace exposures, or high-level dietary contaminations in certain areas (eg, aflatoxin). Background levels of adducts in human DNA range on the order of 1 adduct in 108 nucleotides to 1 in 106 In smokers, reported carcinogen-specific DNA adduct levels are in the upper part of this background range (Marnett and Burcham 1993) The same conclusion can be drawn from animal experiments performed under exposure-controlled conditions In rats treated with aflatoxin B administered in the drinking water, at a dose level which would have resulted in a 50 % induction of liver tumors, the steady-state adduct concentration in liver DNA was shown to be about 1 in 106 (Buss et al 1990). This level of DNA adducts is on the order shown in DNA of humans not specifically exposed to carcinogens Therefore, background adduct levels could well be high enough to make a relevant contribution to the overall cancer incidence A quantitative assignment appears to be premature, however, because the biological significance of the various types of background DNA damage is insufficiently known” [27]. And in neuroscience field: article Mindset kinetics and Some Depression Status: A New Quantitative Model under Biochemical-Toxicology Approach: “Is relevant to introduce new more objective way to the definition of depression status to be pharmacologically treated to be separated to the subject that take advantages with other non-pharmacological strategies. In this kind of disorder also mindset kinetics and their specific limits must be considered to evaluate in objective way saturation situation of the system, specific buffer properties and resilience abilities of individuals. In actual scenario a better objective way to verify the amount of stressing condition, time of exposure and quality must be introduced. A useful instrument for healthcare professionals and patients (using also a toxicological approach: what toxic condition, amount and time of exposure and under a biochemical aspect (kinetics, max velocity of a system, saturation) and not only the receptorial status” [29].
Patki G et al: “Biochemical data suggests that heightened anxiety-like behavior and aggression is associated with increased plasma levels of corticosterone and elevated oxidative stress. Significant alterations in dopamine (DA), norepinephrine (NE) and epinephrine (EPI) were observed within the hippocampus, amygdala, and the prefrontal cortex, suggesting potential involvement of dopaminergic and noradrenergic systems in regulation of aggressive behaviors” [30] (Figure 15).
Figure 15: Mindset kinetics and Some Depression Status: A New Quantitative Model Under Biochemical-Toxicology Approach? J of Pharmacol & Clin Res. 2019.
And relate time of pathological event acute or delayed:
According N Engl J Med. 2017. Jul 6; 377(1): 41-51. “Coronary spasm is also a cause of cardiac arrest, particularly in male smokers with minimal or no pre-existing CAD. Mitral valve prolapse in female patients with ECG repolarization abnormalities, and frequent complex ventricular ectopy, has also been associated with out-of-hospital cardiac arrest. An association between air pollution (fine particulate matter with an aerodynamic diameter <2.5 μm and ozone) and out-of-hospital cardiac arrest has recently been demonstrated. There is a circadian variation in SCD. The peak incidence of SCD occurs between 6 am and noon (and is blunted by beta-blockers), with a smaller peak occurring in the late afternoon for out-of-hospital VF arrests. The incidence is highest on Mondays. In the young (<35 years), the most common cause of SCD is arrhythmia, mostly in the context of an apparently normal heart. The most common causes of SCD are congenital abnormalities in those aged 0–13 years, primary arrhythmia in the 14–24-year age group, and CAD in those >25 years. In 5–20 % of cases no significant cardiac abnormality is found at autopsy” [31].
David C Wraith et al: “Tissues of the CNS, such as the brain, optic nerves, and spinal cord, may be affected by a range of insults including genetic, autoimmune, infectious, or neurodegenerative diseases and cancer. The immune system is involved in the pathogenesis of many of these, either by causing tissue damage or alternatively by responding to disease and contributing to process of repair. It is clearly vital that cells of the immune system patrol the CNS and protect against infection. In contrast to other tissues, damage caused by immune pathology- disease in the CNS can be irreparable. The immune system is involved in the pathogenesis of many of these, either by causing tissue damage or alternatively by responding to disease and contributing to process of repair. It is clearly vital that cells of the immune system patrol the CNS and protect against infection. In contrast to other tissues, damage caused by immune pathology- disease in the CNS can be irreparable. The nervous and immune systems have, coevolved to permit effective immune surveillance while limiting immune pathology we will consider aspects of adaptive immunity in the CNS- brain and the retina, both in the context of protection from infection as well as cancer and autoimmunity, while focusing on immune responses that compromise health and lead to significant morbidity [32]. and according : Activation of the Aryl Hydrocarbon Receptor by Structurally Diverse Exogenous and Endogenous Chemicals* Annual Review of Pharmacology and Toxicology: “The induction of expression of genes for xenobiotic metabolizing enzymes in response to chemical insult is an adaptive response found in most organisms. In vertebrates, the AhR is one of several chemical/ligand-dependent intracellular receptors that can stimulate gene transcription in response to xenobiotics. The ability of the AhR to bind and be activated by a range of structurally divergent chemicals suggests that the AhR contains a rather promiscuous ligand binding site. In addition to synthetic and environmental chemicals, numerous naturally occurring dietary and endogenous AhR ligands have also been identified. In this review, we describe evidence for the structural promiscuity of AhR ligand binding and discuss the current state of knowledge with regards to the activation of the AhR signaling pathway by naturally occurring exogenous and endogenous ligands” [33]. Life Sciences Volume 53, Issue 1, 1993, Pages 1-19 Endogenous and exogenous modulation of gap junctional intercellular communication: Toxicological and pharmacological implications.
E. Trosko et al: “During the evolution of single-celled organisms to multicellular metazoans, a family of highly conserved genes coding for proteins (connexins), which as hexameric units (connexons), has evolved to form intercellular channels (gap junctions). These gap junctions allow ions and small molecular weight molecules to flow between coupled cells, thereby facilitating synchronization of electrotonic or metabolic cooperation. Control of cell proliferation, cell differentiation and adaptive responses of differentiated cells have been speculated to be biological roles of gap junctions. The regulation of these gap junctions can occur at the transcriptional, translational and posttranslational levels. Transient downregulation by endogenous or exogenous chemicals can bring about adaptive or maladaptive consequences depending or circumstances. Stable abnormal regulation of gap junction function has been associated with the activation of several oncogenes. Several tumor suppressor genes have also been associated with the up-regulation of gap junction function. Since gap junctions exist in all organs of the multi-cellular organisms, the dysfunction of these gap junctions by various toxic chemicals which have cell type/tissue/organ specificity could bring about very distinct clinical consequences, such as embryo lethality or teratogenesis, reproductive dysfunction in the gonads, neurotoxicity of the CNS system, hyperplasia of the skin, and tumor promotion of initiated tissue. Understanding how many non-mutagenic chemicals might alter. Normal gap junction function should form the basis of “epigenetic” toxicology. On the other hand, restoring normal gap junction function to cells which have dysfunctional intercellular communication could be the basis for a new approach for therapeutic pharmaceuticals” [34].
Deng B et al: “An analysis of the peripheral nervous system in SOD1-G93A mice revealed that:Schwann cells and axons in mutant mice underwent changes that were similar to those seen in the control mice during the early development of peripheral nerves. The peripheral nerves of SOD1-G93A mice developed progressive neuropathy, which presented as defects in axons and myelin, leading to difficulty in walking and reduced locomotor capacity at a late stage of the disease. Macrophages were recruited and accumulated, and nerve injury and a deficit in the blood-nerve barrier were observed.
Proliferation and the inflammatory micro-environment were inhibited, which impaired the regeneration and remyelination of axons after crush injury in the SOD1-G93A mice. The mutant human SOD1 protein induced axonal and myelin degeneration during the progression of ALS and participated in axon remyelination -regeneration in response to injury” [35].
Ross MK et al: “Chemical atherogenesis is an emerging field that describes how environmental pollutants and endogenous toxins perturb critical pathways that regulate lipid metabolism and inflammation, thus injuring cells found within the vessel wall. Despite growing awareness of the role of environmental pollutants in the development of cardiovascular disease, the field of chemical atherogenesis can broadly include both exogenous and endogenous poisons and the study of molecular, biochemical, and cellular pathways that become dysregulated during atherosclerosis. This integrated approach is logical because exogenous and endogenous toxins often share the same mechanism of toxicity. Chemical atherogenesis is a truly integrative discipline because it incorporates concepts from several different fields, including biochemistry, chemical biology, pharmacology, and toxicology. This review will provide an overview of this emerging research area, focusing on cellular and animal models of disease” [36].
Stancel GM et al: “Many naturally occurring and man-made chemicals present in the environment possess estrogenic activity. Examples include plant and fungal products, pesticides, plasticizers, and other agricultural and industrial chemicals. These environmental estrogens as well as endogenous ovarian estrogens are thought to initiate their physiological actions in target tissues largely via interactions with a nuclear receptor system. The resultant estrogen-receptor complex in turn affects transcription via its interactions with nucleotide sequences known as estrogen response elements (EREs) present in the regulatory regions of hormone responsive genes. A “consensus” ERE sequence GGTCAnnnTGACC was originally identified in the vitellogenin genes of birds and amphibians, but it is now clear that most naturally occurring EREs differ from this sequence in one or more bases. We and others have obtained both in vivo and in vitro data suggesting a differential interaction of receptor complexes containing different ligands with the multiple EREs present in mammalian systems. This raises the possibility that the toxicity of environmental estrogens may arise in part from a differential pattern of ERE activation by environmental compounds relative to endogenous ovarian estrogens. The experimental basis for such a paradigm and its toxicological implications are discussed in this paper” [37].
Swenberg JA et al: “There is a strong need for science-based risk assessment that utilizes known data from diverse sources to arrive at accurate assessments of human health risk. Such assessments will protect the public health without mandating unreasonable regulation. This paper utilizes 30 years of research on three “known human carcinogens”: formaldehyde, vinyl chloride (VC), and ethylene oxide (EO), each of which forms DNA adducts identical to endogenous DNA adducts in all individuals. It outlines quantitative data on endogenous adducts, mutagenicity, and relationships between endogenous and exogenous adducts. Formaldehyde has the richest data set, with quantitative data on endogenous and exogenous DNA adducts from the same samples. The review elaborates on how such data can be used to inform the current risk assessment on formaldehyde, including both the biological plausibility and accuracy of projected risks. Finally, it extends the thought process to VC, EO, and additional areas of potential research, pointing out needs, nuances, and potential paths forward to improved understanding that will lead to strong science-based risk assessment” [38].
Marnett LJ et al: “In humans, approximately 10(7) cells divide per second. Estimates suggest that spontaneous mutations arise in about a third of those cells. These mutations arise as mistakes in DNA replication and when DNA polymerases copy damaged templates. The latter result from chemical hydrolysis of nucleoside bases or by reaction of DNA with electrophiles or reactive free radicals generated during metabolism (endogenous DNA damaging agents). This article highlights recent discoveries and emerging opportunities in the study of endogenous DNA damage and mutation” [39].
Hussain SP et al: “Mutations of the p53 tumor suppressor gene are found in about 50% of all human cancers. The p53 mutation spectra in these cancers are providing clues to the etiology and molecular pathogenesis of cancer. Recent studies indicate that the p53 protein is involved in several vital cellular functions, such as gene transcription, DNA synthesis and repair, cell cycle arrest, senescence and programmed cell death. Mutations in the p53 gene can abrogate these functions and may contribute to genomic instability and progression to cancer. Characteristic p53 mutation spectra have been associated with dietary aflatoxin B (1) (AFB (1)) exposure and hepatocellular carcinoma (HCC); sunlight exposure and skin cancer; and cigarette smoking and lung cancer. The mutation spectrum also reveals those p53 mutants that provide cells with a selective clonal expansion advantage during the multistep process of carcinogenesis. Although a number of different exogenous carcinogens have been shown to selectively target p53, pieces of evidence supporting the endogenous insult of p53 are accumulating. Furthermore, analysis of a characteristic p53 mutation load in nontumorous human tissue can indicate previous carcinogen exposure and may identify individuals at an increased cancer risk”.
Discussion
Many pathological process are strictly linked to endogenous local environmental conditions time related. Iper-bilirubinemia in newborn and ASD, Glicosilation in diabetes, lipids in Atersoclerotic process. Neuronal cell inclusion in Amyotrofic lateral sclerosis and Dementia, the Metastatic process Oxidative stress in some cancer in example due by Cr (VI) and many other example show an undeniable role of Esogenous but also by endogenous factors. Literature report that Hypoxia-inducible factors (HIFs) activate the transcription of target genes that are involved in many aspects of breast cancer progression, such as angiogenesis, metabolic reprogramming, local tissue invasion, and metastasis. So not only the external toxic factors but also endogenous products (of metabolism, catabolism, related to an oxidative process) can start a pathological process. Often exogenous and endogenous toxins often share the same mechanism of toxicity. Observing the major presentation of some bowel cancer is possible to think in an increased probability of causes related to the topographic and local environment situation time related? The fact that all bowel cell present the same genotype and the same probability to develop a cancer but it only present first in determinate places seem to show the presence of other factors linked to a topographic Local environment time related condition. (The same probability and statistics show this).
If P= PROBABILITY OF CANCER EVENT and P= n/N (N = EVENT CANCER)
0 In example if pulmonary cancer start from 1 lobe for this lobe P= 1 for the other P= not 1 So related this consideration Depurative measure can contribute in global treatment if added to the classic therapy? Is possible to introduce new strategy (in example and antidotic –poison relationship) re- considering toxicological properties also by endogenous substanties? In order to more adequately research on this field is relevant to introduce and submit a new scientific discipline named ENDOGENOUS TOXICOLOGY. In this way observing some pathological phenomena under a new light is possible to produce a global better response. To reduce concentration of some endogenous dangerous factors is possible to think in different strategies like: • Reduce syntetic process of endogenous toxic molecule of movens • Increase this catabolic process • Inactivate this subtancties • Remove the toxic substanties • Accelerate elimination • Reduce compelxive time of actions • Use of an antidothe remedy • Use a depurative strategy. • But also other useful to change the frame of the topographic global methabolism-catabolism. A new scientific discipline named ENDOGENOUS TOXICOLOGY must be introduce as an useful instruments to better clear some pathological process and also to introduce better and new pharmacological (and not) strategies. What is relevant is to consider some pathology under a toxicological aspect and endogenous process time related. (Topographic condition, time of exposure, catabolic status). A better knowledge related basic pathologic process make possible to verify and introduce new therapeutic strategies to achieve better global clinical results. Concepts from toxicological sciences like dosage, time of exposure, kinetics, metabolism, dynamics and other must be applied also in endogenous toxicological–pathological process. Like classic toxicology science concept like: − Endogenous local Toxic substantives − Topography of the toxic process − Metabolism-catabolism of this toxics − Measure methods − Kinetics, dynamics − Dose- response relationship − Risk factors − Worsening local endogenous conditions, Additive condition − Preventing strategies − Depurative methods, inactivating methods − Antidotes approach − And other must be used also in this new scientific discipline. Clarifications This works is produced under a pharmacological–toxicological point of view and with no any diagnostic or therapeutic intent, only to produce new research hypotesys.Conclusion
References